
An AC injury is a common one among both professional athletes and weekend sporting warriors.
Not to be confused with a shoulder dislocation, an AC injury is also known as a shoulder separation.
Occurring in the acromioclavicular (AC) joint – hence the AC acronym – an AC injury is usually caused by blunt force to the tip of the shoulder.
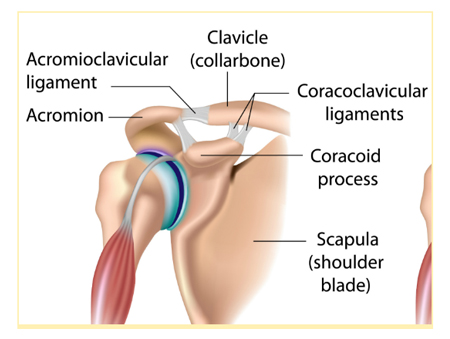
The AC joint is surrounded by a joint capsule and supported by acromioclavicular and coracoclavicular ligaments.
Effectively destabilising these ligaments, an AC injury can be identified when the clavicle detaches from the acromion. You can see where this would occur in the image below.
How do you know if you have an AC injury?
Typical AC joint separation symptoms are shoulder instability and pain.
Another symptom frequently associated with an AC injury is a pronounced bump or bulge at the joint line at the top of the shoulder, like the one shown in the images below. This is a grade V dislocation requiring surgical repair.

Patients usually experience physical symptoms when making movements above the head, like putting on a shirt or reaching into a cupboard, or across the body, such as playing a shot in tennis.
Discomfort during sleep is also commonly reported.
Who gets an AC injury?
Anyone can incur an AC injury.
That said, and while age is not a limiting factor, AC injuries are common in cyclists and footballers. Think about those athletes and weekend warriors I mentioned earlier.
It’s easy to see why they end up with an AC injury when you think about the movements they make.
Tackling in a rugby match, a footballer receives a direct blow to the shoulder.
If a cyclist is unlucky enough to fall from their bike, it’s their shoulder that often takes the brunt of the fall.
Another common occurrence is when people use their hand to break a fall doing everyday life.
When people come to me with an AC injury, one of the first questions they’ll ask me is: Is an AC injury serious?
And my answer to that is no and yes.
An AC injury is not life-threatening, but it can be awkward, uncomfortable and problematic, especially if it’s not identified accurately and early on.
Early, correct diagnosis and treatment timing make all the difference to a patient’s outcome when it comes to an AC joint injury.
Surprisingly, this is a little tricky. Let me explain why.
What about treatment for an AC injury?
In the first instance, most people with an AC injury will present at a hospital accident and emergency (A&E) unit.
A sensible first step, it’s here the AC injury can be identified and x-rayed.
And while this sets a patient on the road to recovery, what’s tricky with an AC injury is the way they’re graded.
Here’s how the grading system works:
There are six grades, from Grade I to VI.
Grade I and II indicate minimal disruption to the AC joint. Essentially a sprain, typical treatment would include cross taping, ice, sling and physiotherapy.
Grades IV to VI are typically best treated with surgical repair. These injuries often cause pain and deformity and commonly affect the long term function of the shoulder.
This leaves Grade III injuries, which fall into a grey area. That grey area means there is considerable debate among clinicians about how these injuries should be treated.
My strong recommendation?
A review by a specialist who deals with these injuries all the time is your best first move, i.e. a specialist shoulder surgeon.
He or she will perform an in-depth functional profile, examination and review of x-rays. Together with their specialised experience in this treatment area, they’ll be well positioned to inform a wise treatment decision. This assessment will determine whether surgical intervention may be the recovery pathway forward.
The grading system is helpful but know that it is subject to the treating physician’s experience with diagnosis.
Working in the first line of assessment (and perhaps not seeing injuries like this all the time), the A&E physician could underestimate or misinterpret the AC injury severity, even with x-rays.
As a result, patients can sometimes be sent away without all the information. Long term, this can cause complications, including the need for surgery, which could have been avoided.
If not assessed correctly within two weeks of the injury, what could have been treated with repair work, such as cross taping, ice, and physiotherapy, has escalated to surgical reconstruction requiring tendon grafts.
In this surgery, donor tissue is used. A tendon taken is from another part of the body, (for example, the hamstring), thereby allowing reconstruction of the ligaments around the AC joint.
What do you really need to know about an AC injury?
If there’s one thing I’d love you to take away from this blog, it’s this:
early and correct diagnosis is pivotal to achieving the most ideal recovery outcome from your AC injury.
If you suspect you have an AC injury, or have been diagnosed and feel uncertain about next steps, be sure to ask your treating physician for more information. This is essential if you want to avoid complications down the track.
Any treatment involving surgery should consider how the repair technique will preserve your shoulder, while also rebuilding the key ligaments that have been torn.
Concerned and want to know more?
Get in touch with the Focus Shoulder Specialist team. We can help you navigate all aspects of diagnosis, treatment and recovery from shoulder conditions.
Dr Sommit Dan is a leading Adelaide shoulder specialist. He provides minimally invasive and more complex treatment for all shoulder injuries and conditions. An Australian trained orthopaedic surgeon and highly skilled in arthroscopic (keyhole) shoulder reconstructions, rotator cuff repair and shoulder replacement surgery, Dr Dan treats patients as people. His goal is to his patients navigate the frequently challenging roadmap to recovery, empowering them along the way.
